
As an organization with nationwide reach, we recognize our work occurs on traditional Indigenous territories across Canada. Arthritis Society Canada’s national office is located in Toronto (Tkaronto), which is the traditional territory of many nations, including the Mississaugas of the Credit, the Anishinaabeg, the Chippewa, the Haudenosaunee and the Wendat peoples.
We also acknowledge that Toronto is covered by Mississauga Treaty 13 (1805) with the Mississaugas of the Credit, and the Williams Treaties (1923) signed with seven Mississaugas and Chippewa First Nations.
We acknowledge this land is now home to many diverse First Nations, Inuit, and Métis peoples.
Pronunciation Guide:
- Mississaugas (mis-sus-SOG-guz)
- Anishinaabeg (ah-nish-in-NAW-beg)
- Chippewa (CHIP-uh-waa)
- Haudenosaunee (HOE-den-no-SHOW-nee)
- Wendat (wen-dat)
- Métis (MAY-tee)
- Inuit (IN-ooh-eet)
Land acknowledgements are acts of Reconciliation, and a way for Canadians to recognize the ongoing injustices and resilience of Indigenous peoples across Canada.
In the land acknowledgement, we acknowledge the land and the waters, the nations of people who are the stewards of these lands. Land acknowledgements also play an important role in treaty education as the treaties are the foundation to the relationship between Canada and First Nations.
These acknowledgements are also a reminder of the responsibility we all have to educate ourselves and address, acknowledge, and repair these injustices.
An important aspect of land acknowledgements is to consider actionable steps towards reconciliation with Indigenous peoples.
We encourage you to learn more about the nations, the land, and the communities in the areas where you live. It is important to understand the impacts of colonization and work together to address these impacts collaboratively with Indigenous peoples.
Arthritis and Indigenous Communities
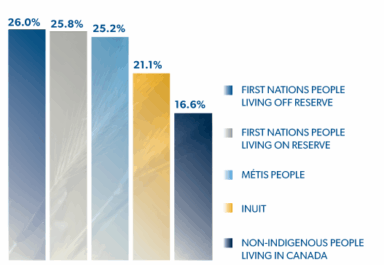 While epidemiological data on the burden of arthritis in Indigenous populations in Canada are limited, arthritis has been found to be more common in First Nations and Métis adults relative to the prevalence among non-Indigenous adults. The Public Health Agency of Canada’s Key Health Inequalities in Canada: A National Portrait (2018) reported the prevalence of arthritis among First Nations people living off reserve (26.0%), First Nations people living on reserve (25.2%), Métis people (25.8%), Inuit (21.1%), and non-Indigenous people (16.6%) living in Canada.
While epidemiological data on the burden of arthritis in Indigenous populations in Canada are limited, arthritis has been found to be more common in First Nations and Métis adults relative to the prevalence among non-Indigenous adults. The Public Health Agency of Canada’s Key Health Inequalities in Canada: A National Portrait (2018) reported the prevalence of arthritis among First Nations people living off reserve (26.0%), First Nations people living on reserve (25.2%), Métis people (25.8%), Inuit (21.1%), and non-Indigenous people (16.6%) living in Canada.
A literature review conducted by Arthritis Society Canada also identified common barriers that Indigenous people face when accessing healthcare, including financial, geographic, social, and political issues. Key barriers highlighted include limitations in healthcare infrastructure, lack of quality of care, social discrimination and cultural obstacles, and more. If you would like to learn more about this internal report, please contact our Mission department at [email protected].
Arthritis Society Canada is currently working diligently with partners at the Arthritis Community Research and Epidemiology Unit (ACREU) based at the University Health Network to shed additional light on the prevalence and impact of arthritis in Indigenous peoples in Canada.
Arthritis Society Canada Actions
Inclusion, Diversity, Equity and Access (IDEA) Working Group
In furtherance of our mission and strategic priorities, we are committed to promoting inclusion, diversity, equity, and access through our information and support, advocacy, innovation, programming, staff and volunteer training, internal policies, and governance structures. In furthering the goals of this work, we aim to ensure that our people reflect the knowledge, experience, skills and diversity (including but not limited to diversity of gender, race, and geographical location) of the communities we live in and serve. This work includes engaging community partners and stakeholders for support, guidance, and training.
Nationwide Social Impact Program
Arthritis Society Canada launched a social impact program in 2021 to work and collaborate with clinicians and researchers to implement transformative and sustainable solutions. The program enables partners to test and refine approaches, services and technologies and scale them across the country to have a positive impact on arthritis. Further details will be released soon.
Community Action Grants Program
Community Action Grants provide opportunities for people to connect, learn, and thrive with arthritis in their own communities. These grants support communities exploring local solutions, where groups and individuals address arthritis-related needs specific to their communities – including health inequities and disparities that impact access to arthritis information and care. Indigenous communities are among specific priority groups that this program is designed to reach.
Below includes a list of Indigenous community initiatives that received funding through the Community Action Grants:

Igloolik Health Centre, Igloolik, Nunavut. In-person group sessions were held in a peer-to-peer format. The program was led by two community health representatives, who delivered arthritis education in Inuktitut. All content was delivered by Inuit, for Inuit, using culturally relevant information; A funding commitment of $2,500 was allocated for this program.
Swan River and District Community Resource Council, Inc. Swan River, Manitoba. Monthly drop-in style arthritis and health-related education and social events were held for the community of Swan River and other sites in Wuskwi Sipihk First Nation in northwest Manitoba. The sessions included discussion with local healthcare professionals and subject matter experts; A funding commitment of $5,000 was allocated for this program.

Manitoba Métis Federation, Winnipeg, Manitoba. A speaker series on arthritis education and self-management for Red River Métis citizens in Winnipeg. Each in-person session paired discussions of scientific evidence with Métis ways of knowing. Local subject matter experts lead sessions, including a Métis Elder who shared traditional approaches to healing and coping with arthritis symptoms; A funding commitment of $5,000 was allocated for this program.
For more details, please visit our webpage Community Action Grants.
Research Initiatives
Arthritis Society Canada is Canada’s largest charitable funder of cutting-edge arthritis research. The investments we make in research and discovery seek to spark new ideas and careers in arthritis research. Here are some of the research projects and programs involving Indigenous populations and communities that have been supported by Arthritis Society Canada donors:
As a PhD student, Dr. Vidyanand Anaparti (University of Manitoba) studied how rheumatoid arthritis starts in children from Indigenous communities in northern Manitoba who have a high risk of developing the disease, focusing on the role of molecules that act as “switches” to turn genes on and off.
As an early career investigator, Dr. Glen Hazlewood (University of Calgary) focused on understanding treatment and disease management preferences among patients with rheumatoid arthritis as well as healthcare providers. This included research specifically focused on the perspectives of patients in southern Alberta from First Nations or Métis communities, highlighted as a Top 10 research advance in 2019. By bridging the gap between treatments physicians recommend, and those that patients want, Dr. Hazlewood’s work is informing best practices in clinical decision-making.
Dr. Diane Lacaille (University of British Columbia and Arthritis Research Canada) led her team to develop a novel model of care to respond to the needs of First Nations people living with arthritis. It aimed to facilitate culturally safe care and foster the development of care plans that integrated the management of arthritis with that of other chronic conditions. This model was supported by a nurse case manager who resided in the community. The model of care was guided by a needs assessment with community members and the case managers acted as effective community liaisons.
Dr. Brian Feldman (University of Toronto) initiated the development and study of a new model of community-based care for children with arthritis in Ontario, toward improving access to care – especially for underserved Northern, rural and Indigenous populations. This involved having highly skilled physiotherapists and occupational therapists see children with arthritis in their own communities or through traveling clinics in remote locations, including on reserves. The practitioners then consulted with a pediatric rheumatologist via telemedicine. This resulted in pilot clinics in two underserved Ontario locations in Thunder Bay and Windsor, leading to a monthly clinic established in Thunder Bay.
Based at the University of Calgary, Dr. Cheryl Barnabe, rheumatologist and member of the Métis Nation of Alberta, worked with her team to establish an arthritis screening and specialty care program in a primary healthcare centre for Indigenous patients in Calgary (Elbow River Healing Lodge). The goals were to deliver care in a new way to Indigenous patients, remove barriers to care access, and treat patients holistically to achieve recognized treatment standards. This patient-centred model of care resulted in high patient satisfaction and enhanced diagnosis.
Dr. Christine Peschken (University of Manitoba) led researchers from the Canadian Network for Improving Outcomes in Systemic Lupus Erythematosus (CaNIOS) to produce several discoveries on what lupus looks like and how it acts, through the ‘1,000 Canadian Faces of Lupus’ project. This included research on the burden and impact of lupus in First Nations people in Canada.
For more information about our research and its impact, please visit: www.arthritis.ca/research
We would like to thank Bob Goulais of Nbisiing Consulting for their organization-wide support in land acknowledgements, and Toronto for All / Toronto Aboriginal Support Services Council for their resources.
